I was hoping to receive some information/insight on the process for midshipmen who were accepted to the medical corps after graduation, finished medical school, and are in the process of applying to residencies. I was told by a USMA grad in his final year of residency that some of his Navy USUHS and HPSP alumni colleagues applied to their residencies, were then forced to serve on a ship for an undisclosed amount of time, and then had to reapply to residency again. Is this the norm for all Navy USUHS and HPSP graduates?

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
- Joined
- Sep 27, 2008
- Messages
- 20,564
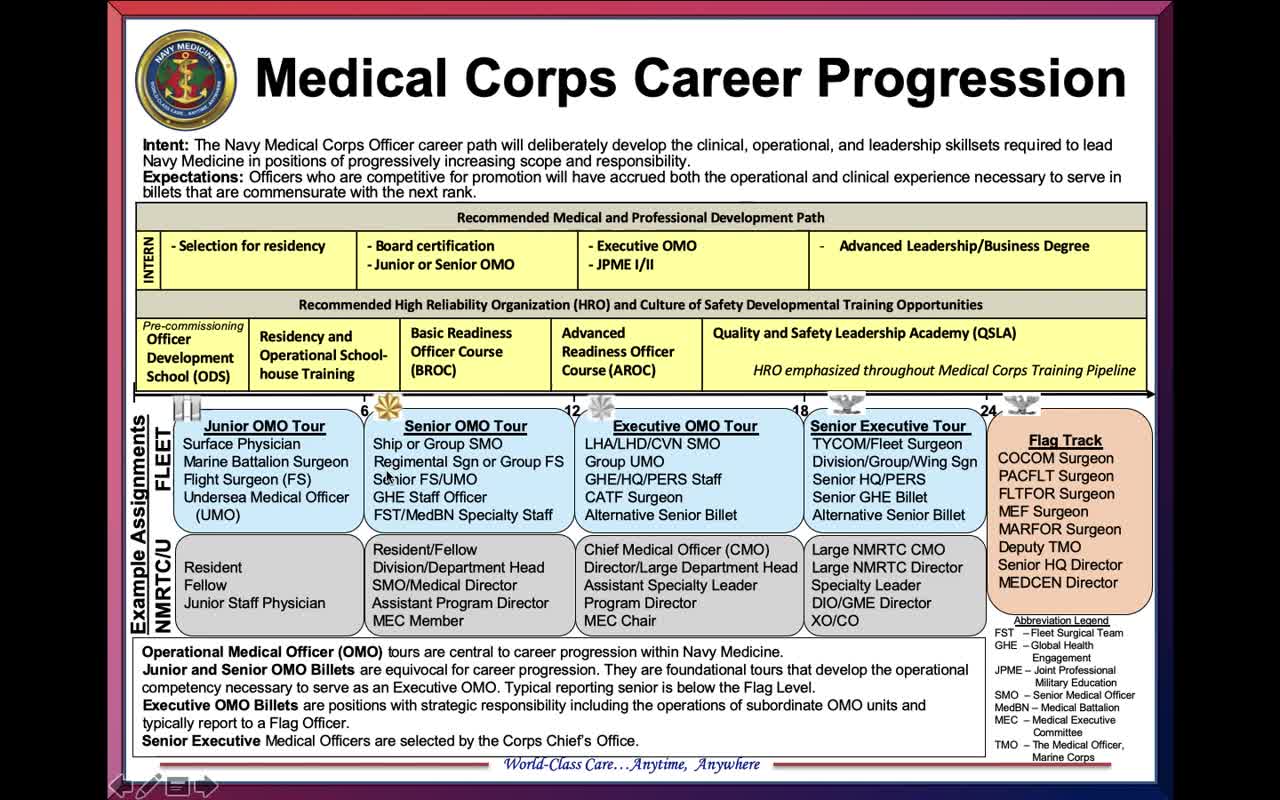
I’ve inserted a link below for a well-known blog on Navy Medical Corps careers, therefore unofficial, but it does have links to the latest official MC career path infographic pdf.I was hoping to receive some information/insight on the process for midshipmen who were accepted to the medical corps after graduation, finished medical school, and are in the process of applying to residencies. I was told by a USMA grad in his final year of residency that some of his Navy USUHS and HPSP alumni colleagues applied to their residencies, were then forced to serve on a ship for an undisclosed amount of time, and then had to reapply to residency again. Is this the norm for all Navy USUHS and HPSP graduates?
The last year has brought the term “operationally relevant” to the forefront as a career progression driver. The Navy is a sea-going service, and the Marine Corps is right there beside them. MC officers are Navy officers first, staff corps officers second, and are expected to be corporately literate on their Service and the Corps. Medical staff who are familiar with the Fleet and Corps in actual operational settings, who live as part of ship’s company, soak up valuable knowledge on sailors and Marines, the culture, the challenges, the dangers of life at sea. It’s you and your corpsmen with a thousand miles of blue water between you and the nearest medical facility (though carriers have pretty cool med gear). You will also get to know and respect that storied breed, the IDC, the Independent Duty Corpsman, found on the ships and subs who are not large enough for a Med Corps officer onboard, and who go into battle with Marines. Cue @Devil Doc
There are interesting things that can be done. One of our USNA sponsor family mids went the USUHS route and was assigned to an Undersea Warfare Command. He was usually with the SEAL/UDT teams, got qualified as a Navy diver, went out on training and ops with them doing Interesting Stuff. He loved that tour, made him feel like he was part of the operational Navy, and that non-medical professional knowledge and insight have benefited him greatly over the years. He is wrapping up his ortho residency right now and doing very well. Another one went to the medical treatment facility (MTF) in Naples, Italy, was often sent out for short periods on ships in the Med (port calls in Palma! Malaga! Palermo! Marseilles!) and up to Germany to the major medical centers there, and he took full advantage of the tremendous travel opportunities before rollling into his residency stateside.
Anyone who goes into Navy medicine out of USNA or NROTC or via the HPSP is in it for the long haul due to the years of active duty service obligation. Anyone who is dismayed by “being forced to serve on a ship” should thoughtfully reflect on career paths involving the Navy.
The New Medical Corps Career Progression Slide – What Does It Mean to You?
Navy Medicine has been undergoing a lot of change. We have a new Surgeon General, a new Corps Chief, and a renewed focus on readiness. With these changes come a new career progression and path for …
 mccareer.org
mccareer.org
Thank you very much!I’ve inserted a link below for a well-known blog on Navy Medical Corps careers, therefore unofficial, but it does have links to the latest official MC career path infographic pdf.
The last year has brought the term “operationally relevant” to the forefront as a career progression driver. The Navy is a sea-going service, and the Marine Corps is right there beside them. MC officers are Navy officers first, staff corps officers second, and are expected to be corporately literate on their Service and the Corps. Medical staff who are familiar with the Fleet and Corps in actual operational settings, who live as part of ship’s company, soak up valuable knowledge on sailors and Marines, the culture, the challenges, the dangers of life at sea. It’s you and your corpsmen with a thousand miles of blue water between you and the nearest medical facility (though carriers have pretty cool med gear). You will also get to know and respect that storied breed, the IDC, the Independent Duty Corpsman, found on the ships and subs who are not large enough for a Med Corps officer onboard, and who go into battle with Marines. Cue @Devil Doc
There are interesting things that can be done. One of our USNA sponsor family mids went the USUHS route and was assigned to an Undersea Warfare Command. He was usually with the SEAL/UDT teams, got qualified as a Navy diver, went out on training and ops with them doing Interesting Stuff. He loved that tour, made him feel like he was part of the operational Navy, and that non-medical professional knowledge and insight have benefited him greatly over the years. He is wrapping up his ortho residency right now and doing very well. Another one went to the medical treatment facility (MTF) in Naples, Italy, was often sent out for short periods on ships in the Med (port calls in Palma! Malaga! Palermo! Marseilles!) and up to Germany to the major medical centers there, and he took full advantage of the tremendous travel opportunities before rollling into his residency stateside.
Anyone who goes into Navy medicine out of USNA or NROTC or via the HPSP is in it for the long haul due to the years of active duty service obligation. Anyone who is dismayed by “being forced to serve on a ship” should thoughtfully reflect on career paths involving the Navy.
The New Medical Corps Career Progression Slide – What Does It Mean to You?
Navy Medicine has been undergoing a lot of change. We have a new Surgeon General, a new Corps Chief, and a renewed focus on readiness. With these changes come a new career progression and path for …
- Joined
- Apr 25, 2018
- Messages
- 5,516
@Capt MJ thank you ma’am, I now want to get underway instead of drive up I-95 to work.
@bookthief Independent Duty Corpsmen classify ships as doctor ships or IDC ships. About 80 percent of them are IDC ships but fear not, the ship to which you are assigned will also have an IDC. Carriers have at least five medical officers when the wing is aboard plus two IDCs. I was stationed on three IDC ships and one doctor ship. The doc and I became friends and taught each other things. Medical officers are not “forced to serve on a ship for an undisclosed amount of time.” They are in a service with ships and ships are meant to go to sea. That’s what we do. You would report aboard and already know your date of transfer.
The Marines. Totally different environment and mindset. You’ll look like them and train and deploy with them and the more you act like them the better. I was Green Side as we call it three times. I left shore duty early two times to go back to the Marines. I loved it just as America loves her Marine Corps. I even gave my son away to the Marines. He loves it as well.
@bookthief Independent Duty Corpsmen classify ships as doctor ships or IDC ships. About 80 percent of them are IDC ships but fear not, the ship to which you are assigned will also have an IDC. Carriers have at least five medical officers when the wing is aboard plus two IDCs. I was stationed on three IDC ships and one doctor ship. The doc and I became friends and taught each other things. Medical officers are not “forced to serve on a ship for an undisclosed amount of time.” They are in a service with ships and ships are meant to go to sea. That’s what we do. You would report aboard and already know your date of transfer.
The Marines. Totally different environment and mindset. You’ll look like them and train and deploy with them and the more you act like them the better. I was Green Side as we call it three times. I left shore duty early two times to go back to the Marines. I loved it just as America loves her Marine Corps. I even gave my son away to the Marines. He loves it as well.
- Joined
- Sep 27, 2008
- Messages
- 20,564
If you’re smart, you learn just as much about doctoring in the Navy working beside an IDC as you do on rounds with a top doc during residency. It’s different knowledge but invaluable.
I realized the OP told us the source of his info was a USMA grad, so quite possibly we had a bit of Army horror-of-the-sea bias going on with “forced to serve on a ship for an undisclosed amount of time.”
I realized the OP told us the source of his info was a USMA grad, so quite possibly we had a bit of Army horror-of-the-sea bias going on with “forced to serve on a ship for an undisclosed amount of time.”
Last edited:
- Joined
- Jul 15, 2007
- Messages
- 2,415
As CaptMJ/DevilDoc have discussed, operational experience (afloat and/or FMF) is expected/required from practically every Navy community, including the Staff Corps (Medical, Dental, Supply, Chaplain). It probably would be extremely difficult to promote without it. Linked below is the official/approved Community Briefs (i.e. notional pipelines) for the Navy (Medical Corps can be found in the Staff Corps link on PDF pages 2-3). Hope this helps, as well.
Line (Unrestricted/Restricted): https://www.mynavyhr.navy.mil/Porta...documents/FY-22_Act_Community_Briefs-Line.pdf
Staff Corps: https://www.mynavyhr.navy.mil/Porta...22 Act Community Briefs 13NOV2020 - Staff.pdf
Line (Unrestricted/Restricted): https://www.mynavyhr.navy.mil/Porta...documents/FY-22_Act_Community_Briefs-Line.pdf
Staff Corps: https://www.mynavyhr.navy.mil/Porta...22 Act Community Briefs 13NOV2020 - Staff.pdf
- Joined
- Aug 27, 2010
- Messages
- 5,824
FWIW, when my first ship was being built, our newly assigned Doctor spent most of his time at an Air Force medical facility at Langley AF Base so we didn't get to interact with him very much. Once we moved aboard and became a fleet unit, we found out that he was a Gynecologist by training and this was his fleet tour prior to serving more of his OB/GYN specialty stuff.
NOTE: this was the early 80's and the ship had a 100% male crew.
My second ship had a Doc (USNA grad) who was headed to a Radiology specialty. NOTE: we had no real radiology assets aboard.
NOTE: this was the early 80's and the ship had a 100% male crew.
My second ship had a Doc (USNA grad) who was headed to a Radiology specialty. NOTE: we had no real radiology assets aboard.
FWIW, when my first ship was being built, our newly assigned Doctor spent most of his time at an Air Force medical facility at Langley AF Base so we didn't get to interact with him very much. Once we moved aboard and became a fleet unit, we found out that he was a Gynecologist by training and this was his fleet tour prior to serving more of his OB/GYN specialty stuff.
NOTE: this was the early 80's and the ship had a 100% male crew.
My second ship had a Doc (USNA grad) who was headed to a Radiology specialty. NOTE: we had no real radiology assets aboard.


thanks for the laugh! It’s been a rough week at the clinic and I needed that!
- Joined
- Apr 25, 2018
- Messages
- 5,516
Physicians are trained to use all the modern technology and diagnostic equipment and get a wake up call when they don't have a lot of that aboard ship. IDCs are trained in turn of the century medicine. Turn of the 19th to the 20th century medicine when no CT, MRI, advanced lab and x-ray was available. It was the scariest, most fun, and exciting job I can imagine.FWIW, when my first ship was being built, our newly assigned Doctor spent most of his time at an Air Force medical facility at Langley AF Base so we didn't get to interact with him very much. Once we moved aboard and became a fleet unit, we found out that he was a Gynecologist by training and this was his fleet tour prior to serving more of his OB/GYN specialty stuff.
NOTE: this was the early 80's and the ship had a 100% male crew.
My second ship had a Doc (USNA grad) who was headed to a Radiology specialty. NOTE: we had no real radiology assets aboard.
- Joined
- Aug 27, 2010
- Messages
- 5,824
The Radiologist was the Doc that I taught to do celestial navigation along with shiphandling.Physicians are trained to use all the modern technology and diagnostic equipment and get a wake up call when they don't have a lot of that aboard ship. IDCs are trained in turn of the century medicine. Turn of the 19th to the 20th century medicine when no CT, MRI, advanced lab and x-ray was available. It was the scariest, most fun, and exciting job I can imagine.
Old Navy BGO
10-Year Member
- Joined
- Jan 5, 2012
- Messages
- 4,619
Why am I imaging Devil Doc pouring over a thick IDC handbook, following the diagnosis flowchart , but no matter what the symptoms are, they all lead to the last page where the treatment is " Two Motrin, Hydrate and Change Socks" ?Turn of the 19th to the 20th century medicine when no CT, MRI, advanced lab and x-ray was available. It was the scariest, most fun, and exciting job I can imagine.
")
- Joined
- Sep 27, 2008
- Messages
- 20,564
I thought it was the 800mg Motrin from the huge jar on the steel file cabinet behind the steel desk?Why am I imaging Devil Doc pouring over a thick IDC handbook, following the diagnosis flowchart , but no matter what the symptoms are, they all lead to the last page where the treatment is " Two Motrin, Hydrate and Change Socks" ?
- Joined
- Apr 25, 2018
- Messages
- 5,516
In IDC school the last treatment in a list of treatments was always medevac. E.g. pneumonia- treat with ampicillin, humibid, fluids, bed rest, medevac.Why am I imaging Devil Doc pouring over a thick IDC handbook, following the diagnosis flowchart , but no matter what the symptoms are, they all lead to the last page where the treatment is " Two Motrin, Hydrate and Change Socks" ?
That was in case the treatment didn’t work and the patient needed a higher echelon of care. I always figured it was to cover the school in case we held on to a patient but should have flown them off. Plus, a medevac isn’t always available. I got to BUMED 10 years later and was in charge of the IDC and preventive medicine technician curriculum. I had to answer a congressional inquiry about how the TB skin test was taught in PMT school. There’s a long story that’s more interesting but the short one is it was a good thing the curriculum covered all involved.
Small Team Bacsi
Member
- Joined
- Jul 17, 2020
- Messages
- 1,573
Ships? Navy ships?
I am not sure our USN medical doctor Doctor B spent any time at all on a navy ship during his one tour with the navy and before he became a shrink. So you may be luckily like him And avoid serving on a Navy ship
although the draw back for the good doctor was instead of being on a navy ship he was with the first Marines (1/1 and 3rdRecon) to venture up into the dreadful and very interesting Charlie Ridge. Feb 1966 Operation Taut Bow.
when the NVA first hit us with mortars the good doctor qualified for his Combat Action Ribbon.
Although this was so Old Corps the CAR did not exist yet.
Good Luck
I am not sure our USN medical doctor Doctor B spent any time at all on a navy ship during his one tour with the navy and before he became a shrink. So you may be luckily like him And avoid serving on a Navy ship
although the draw back for the good doctor was instead of being on a navy ship he was with the first Marines (1/1 and 3rdRecon) to venture up into the dreadful and very interesting Charlie Ridge. Feb 1966 Operation Taut Bow.
when the NVA first hit us with mortars the good doctor qualified for his Combat Action Ribbon.
Although this was so Old Corps the CAR did not exist yet.
Good Luck